Discharge Against Medical Advice Form - I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. A form for patients who choose to leave hospital against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. It requires the patient's signature, the doctor's signature and a witness'.
It requires the patient's signature, the doctor's signature and a witness'. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. A form for patients who choose to leave hospital against medical advice.
A form for patients who choose to leave hospital against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. It requires the patient's signature, the doctor's signature and a witness'.
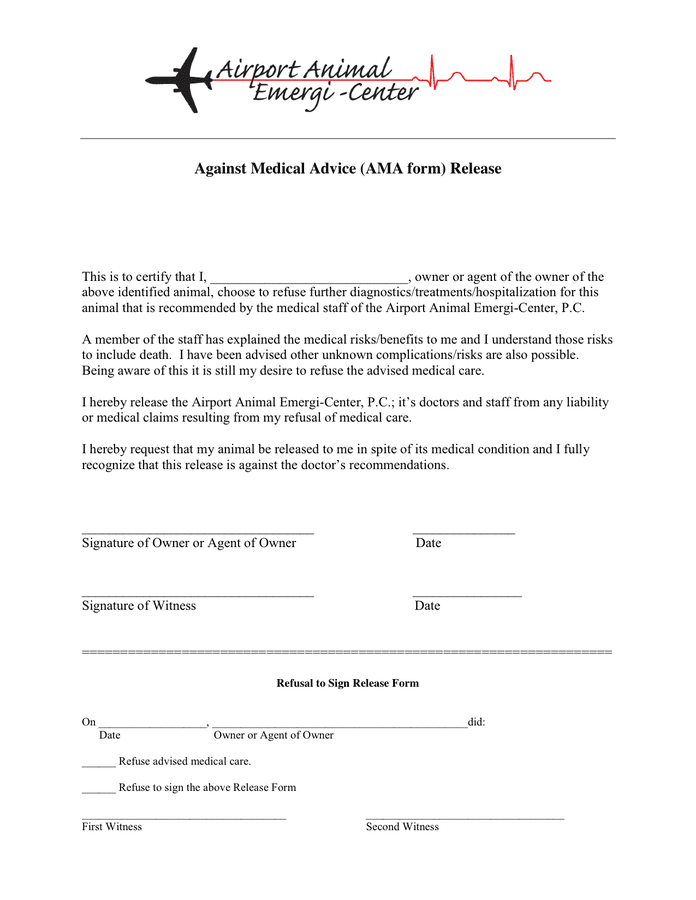
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-37.jpg)
39 Printable Against Medical Advice [AMA] Forms
A form for patients who choose to leave hospital against medical advice. I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. It requires the patient's signature, the doctor's signature.
Against Medical Advice Form download free documents for PDF, Word and
It requires the patient's signature, the doctor's signature and a witness'. I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. A form for patients who choose to leave hospital against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical.
Printable Discharge Against Medical Advice Form Web Against Medical
I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. It requires the patient's signature, the doctor's signature and a witness'. A form for patients who choose to leave hospital.

FREE 8+ Against Medical Advice Forms in PDF
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. It requires the patient's signature, the doctor's signature and a witness'. A form for patients who choose to leave hospital against medical advice. I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks.
8 Free Against Medical Advice (AMA) Forms (Word, PDF)
I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. A form for patients who choose to leave hospital against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. It requires the patient's signature, the doctor's signature.
Against Medical Advice Form download free documents for PDF, Word and
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. It requires the patient's signature, the doctor's signature and a witness'. I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. A form for patients who choose to leave hospital.
FREE 7+ Sample Medical Advice Forms in PDF MS Word
A form for patients who choose to leave hospital against medical advice. I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. It requires the patient's signature, the doctor's signature.
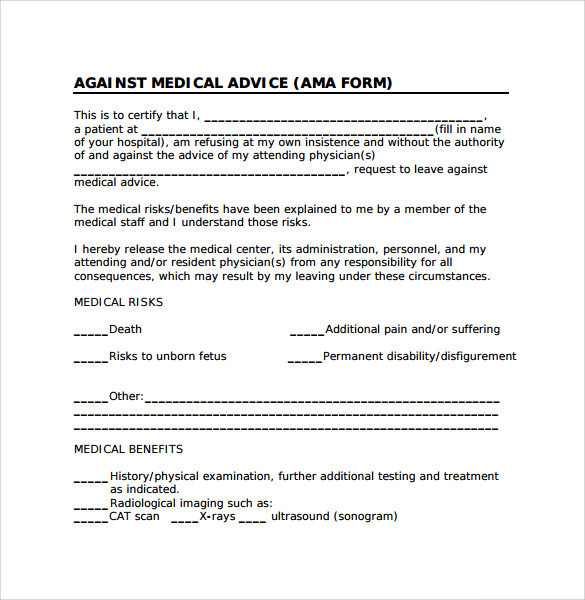
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-26.jpg)
39 Printable Against Medical Advice [AMA] Forms
It requires the patient's signature, the doctor's signature and a witness'. I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. A form for patients who choose to leave hospital against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical.
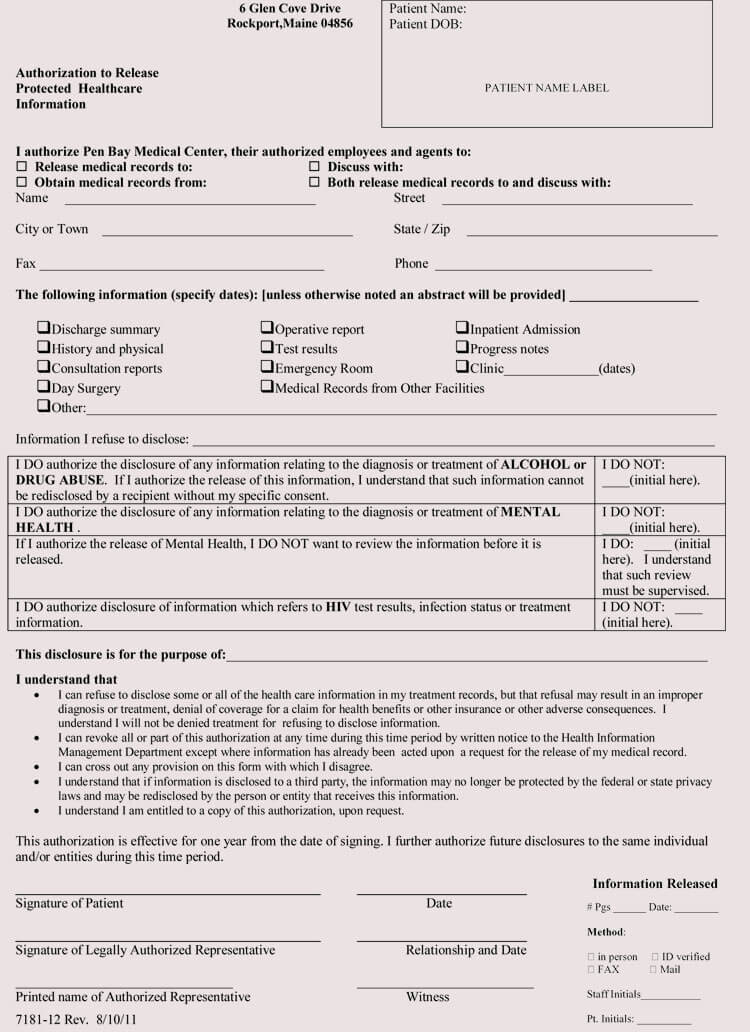
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-28.jpg)
39 Printable Against Medical Advice [AMA] Forms
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. A form for patients who choose to leave hospital against medical advice. It requires the patient's signature, the doctor's signature.
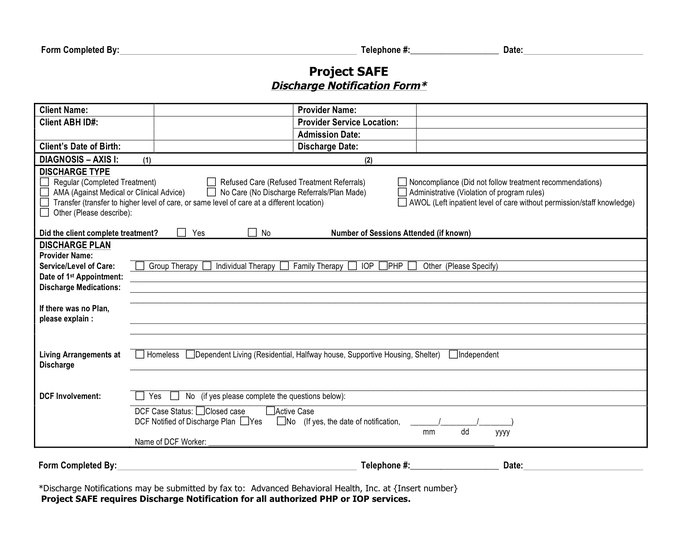
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-01.jpg)
39 Printable Against Medical Advice [AMA] Forms
A form for patients who choose to leave hospital against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I have been advised of the possible dangers to my life or health from this departure, and i hereby assume the risks and consequences involved. It requires the patient's signature, the doctor's signature.
I Have Been Advised Of The Possible Dangers To My Life Or Health From This Departure, And I Hereby Assume The Risks And Consequences Involved.
A form for patients who choose to leave hospital against medical advice. It requires the patient's signature, the doctor's signature and a witness'. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the.